Article No. 398
4 December 2020
In its previous article “Dip into ASH 2020” Global Action highlighted research results relating to “aHUS” and “TMA” which are to be presented at the ASH conference. (see Article 397).
However there was one Oral and Poster Abstract about aHUS that warranted its own report.
Research by the Acosta Medina Group has brought together in a literature review, a summary of the relapse rates of those who have discontinued eculizumab.
Determination of Relapse By Risk by Complement Gene Variants after Eculizumab Discontinuation in Complement Mediated Thrombotic Microangiopathy : A Retrospective Review ( click title to read full abstract)
The article provides the most comprehensive data so far on the risk of withdrawal of treatment based on Complement component genetic variants, or lack of such variants.
However the Group takes one more step to assess the risks WITHIN each Complement component.
It is not just a case of knowing which Complement component is defective but which part of of that component is affected and in what way .
The Groups results came from a search of publications relating to over 500 patients who had been treated with eculizumab. Of them 194 had discontinued eculizumab treatment and had sufficient data available for inclusion. Of the 194 patients, 118 had identifiable genetic variants, 76 were idiopathic.
The overall relapse rate on discontinuation of eculizumab was just less than 29%. 13% of those with no identified genetic variant relapsed, whereas just under 39% of those with genetic variant relapsed.
Readers of this website may be familiar with risk matrix model that Global action has featured from time to time.
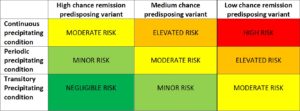
Based on the groups findings those without identified genetic effects would fall into the first column. And those with genetic defects would seem be spread over columns 2 and 3. Though it is not as simple as that.
First of all data is given for each of the Complement component relapse rates.
| Component | Relapse Rate % |
| CFH | 52.5 |
| MCP/CD45 | 45 |
| CFI | 37.5 |
| C3 | 28.57 |
| Other | 33.3 |
| Anti Factor H antibodies | 12.5 |
| Combined | 57.14 |
| Not specified | 0 |
This would suggest that risks for those with CFH , MCP /CD46 and Combined variants would be found more towards the top right hand boxes of above risk matrix.
Those with CFI C3 and other ( DGKE) would be in the middle column and Anti Factor H antibodies in the first column.
Where reported, the Study group has drilled down into the specific variant for each of the Complement components and found that some variants were more likely to cause relapse than others,
Almost all CFH variants were found to be at a higher risk, more than 50% chance of relapse but one on “exon 18” had a 33% relapse rare and of those with CFH variants not specified only 40% relapsed. Moving some with CFH variants into the middle column.
Similar analysis has been carried out for each of the components. Most of the risk for those with MCP/CD46 would be if their variants were found in what is called the “spliced region” – i.e. 83.3% relapse rate. Those with variants elsewhere either had no relapse, or 100% relapse where not specified.
And so on the study goes through each of the components with some variants putting the patients in column 1 whilst others move to column 3.
Other clinical history factors or patient characteristics are at play too and influence relapses.
Relapse is more likely
-with a genetic variant – three times as likely
-with a history of more TMA events – twice as likely
-at age 30 and below- just less than twice as likely
-with more complement variants- slightly more likely
-with CFH variants involve- twice as likely
But a new aHUS event needs a trigger event which is more likely if the trigger is continuous e.g. a kidney transplant, than for periodic or transitory events , the flu or pregnancy.
The science surrounding the withdrawal from eculizumab ( as well as ravulizumab ) treatment is gaining momentum. Eventually it is to be hoped that the risk matrix will be filled up to guide withdrawal decisions and drive informed consent by aHUS patients, including those who will need to remain on treatment.
It is clearly not a binary decision of being in the red or green zones ; there is a spectrum of colours in between and within each of these there are differing shades.
No guarantees can be given just chances.
When it is needed eculizumab ( and ravulizumab) is essential for the treatment of a catastrophic aHUS event, but when not needed it is a waste of precious resource.
Better diagnosis will get eculizumab to patients when they need it most, better understanding of when that need is no more will make treatment more economical for more aHUS patients who need it.
Previous website articles about withdrawal from eculizumab treatment.
RISK OF WITHDRAWAL OF ECULIZUMAB

{kind=link}