Along with the question about withdrawal from Complement inhibitor treatment , aHUS patients consider that research into the state of aHUS remission ,whether ever or never treated with eculizumab , matters to them.
The alliance has featured the major studies on eculizumab withdrawal , including the Ardissino Study in Italy , STOPECU in France , CUREiHUS in the Netherlands and SETS in the U.K. ( although some of these studies have also looked at dose levels to avoid insufficient or excessive eculizumab dose prescription).
But not all experience of eculizumab withdrawal will be captured by these important studies. Many other patients are going through withdrawal, but the knowledge of how they fared may be lost to the aHUS community and be of no benefit to others if nothing is published about it. Even if only as an individual case study.
A recently published article titled:
Atypical haemolytic uraemic syndrome in the eculizumab era: presentation, response to treatment and evaluation of an eculizumab withdrawal strategy
was spotted in ERKNet’s new Journal Watch programme;in particular the section relating to its TMA cluster. ( To see abstract click here)
It is an example of retrospective analytical research and was carried out by the University College of London Hospital.
It looks at the aHUS patients that have been referred to its TMA Expert Centre from a network of hospitals in London and the surrounding South East of England. Since 2011, 34 new onset aHUS patients ( none with a Renal transplant) have entered its care pathway and this research reports on what happened to them.
All referrals with TMAs receive at least 5 days of Plasma Exchange treatment before a diagnosis of aHUS results in a prescription of a Complement inhibitor. 9 of the 34 went into remission with PEX alone and 25 moved onto Complement inhibitors of which 22 received eculizumab.
The analysis reveals that 13 of those receiving treatment eventually, after counselling on risks etc , agreed to stopping treatment. By far and large those stopping had what would be regarded as low risk genetic predispositions or no identifiable genetic cause. After 18 months of follow up three had returned to treatment but two with reasons, which once overcome ,would lead to withdrawal consideration at a later date.
The research analysis has a table which gives important clinical data about each patient and which may explain why they might be capable of remission without treatment. They are not cured ,but with reasonable levels of monitoring, could live safely in that state.
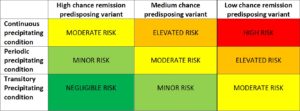
In a few years time all this data will hopefully be brought together to produce a risk matrix which could be used to determine where future patients might fit, and to guide future treatment course .
As has been mentioned many times before it is important that the patient is the one to make the decision, and that that decision needs research data which explains their risk based suitability for withdrawal , and a need for safe monitoring, maybe for a life time. So remission need not be a scary time and one which people can go about their lives with reasonable confidence .
One of the authors of the publication, Prof. Marie Scully ,was one of the members of the aHUS Registry who on Rare Disease Day 2019 gave some words of assurance to the aHUS Patient community about future aHUS research on. Click on the link below the photo graph to hear it.

Prof Marie Scully

{kind=link}