11am 23 June 2022, Bergamo,Italy: The long awaited ISN Frontiers meeting about Renal Complement diseases featuring aHUS is about to begin. Originally intended to be held in 2020 but postponed because of COVID 19 this conference should bring up to date news about aHUS and its treatments over the next three days.
Day 1 opens with a welcome from ISN by Agnes Fogo, USA. “Joyous occasion” she called it as this was ISN’s first face to face meeting since before the pandemic. Events such as these are an important part of ISN’s vision of a future where all people have equitable access to kidney health.
Then it was onto the plenary opening talk by Prof. Guiseppe Remuzzi of the Mario Negri Institute and Co-Chair of the meeting. He explained the complement system and previewed the scientific talks to be presented on the second day of the meeting. One fact about theComplement sysytem “it can lys ( destroy) a bug in 30 seconds”. A powerful tool when used properly.
This was followed by two talks about complement mouse models for research. BB5.1 was mentioned. That mouse was used to develop a monoclonal antibody to block C5, which we now know as eculizumab. ( see more HERE)
The rest of the day was devoted to the other disease of C3G and MPGN. Increasingly it is found that complement plays a part in the disease’s mechanisms and complement inhibitors are being found to control them.
BREAKING NEWS
ISN provide the following link to the virtual session (via Zoom) of the Patient Day: I.e Day 3 https://us06web.zoom.us/j/87874934774
People who will attend the online session will not need to register.
The session will start at 08.30 a.m. (Italian time) on Saturday
Day 2
Begins with research undertaken using mouse models. Firstly one with a CFH mutation ( on SCR20) and aHUS and then one with typical HUS. In each the way in which the two disease develops and this helps elicit potential targets for therapies. One symptom found in the CFH mice was loss of tail caused by aHUS injury , reminiscent of the “COVID toes” co morbidity that has been observed.
Then it is on to genetics. David Kavanagh talked about genetic causes of aHUS in Complement and non Complement mutations ( e.g DGKE ) and how genetic sequencing can help personalise management of aHUS. He mentioned that no large pedigree of CFI has been found unlike CFH and CD46 families.
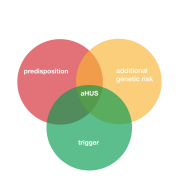
Elena Goicoechea de Jorges’ talk was about the patient ”Complotype” which includes common polymorphisms as well as rare genetic mutations. The polymorphisms may modify the effects of the mutations by putting patients at more risk of or protecting them from an aHUS onset and explain incomplete penetrance in families. Also why some may explain why some have worse kidney injury.
Arvinda Bagga from India gave an online talk about anti factor H autoantibody aHUS. More prevalent in children can affect adults. The antibodies can bind with many parts of CFH. Other complement components also have their own antibodies. Patients are unlikely to have any genetic mutations. Eculizumab is preferred for AFHA treatment but PEX also reduce antibody levels. High antibody and low free CFH are predictors of relapse in 6 to 24 months. PEX and immunosupression improves outcomes. Some improvement in outcomes observed in past 8 years. Donors should also be screened before living donation for transplants.
Next that question “why the kidney? is the subject of Kubka Roumenuria’s talk. It could be the shear stress from the high blood pressure.It could be the structure of the glomurala endolethial cells – fenestrating. It could be a susceptibility to stress factors or some organ specific action of complement.
But they do not explain it. Also here the science in the talk became too complicated for the reporter to explain and it will be looked at and reported in a future blog article. Spoke to Lubka during the interval and will write about her findings separately.
The next talk by Giovanni Montini was about whether it is still necessary to talk about primary and secondary aHUS when it come C5 inhibition. The speaker is a part of the team led by Gianluigi Ardissino in Milan. Gianluigi is well known to Global Action. information was presented about the Milan patients their triggers and their mutations. Triggers overlap but complement mutation only appear in primary. Timing of treatment is important , up to 15 days is rapid , 16 days is or more is delay. Details of the monitoring of treatment withdrawal including self monitoring using urine dips were outlined.”
Raja Ramachandran then talked about pregnancy aHUS. In the past ten years. there has been a halving of prepartum AKI and increase in post partum AKI .Only 8% were aHUS. Lack of awareness , non availability of investigations, late presentations to nephrologists and reluctance to biopsy or scan contribute limitations to diagnosis.Some studies were reported to show that out of many unsuspected aHUS patients all were in fact aHUS patients. There is a high prevalence of CFHR deletions in Indian aHUS pregnancy cases. Most common mutation CFH.
The monitoring of complement disregulation in aHUS was the subject of the final talk of the morning session. The distinction between circulating C5b-9 and its expression on cell surface was explained using the results of a study undertaken by the Mario Negri Institute. Particularly when using the HMEC 1 test. Useful for testing whether eculizumab is doing its job! Will it become common practice? Does it differentiate from other TMAs. Eventually and yes.
Two talks to open the afternoon session both with the same title
14:00 – 14:20 Eculizumab in Primary and Secondary aHUS: Who, When, and How Long?
Sjoerd Timmermans, Netherlands
14:20 – 14:40 Eculizumab in Primary and Secondary aHUS: Who, When and, How Long?
Giuseppe Remuzzi, Italy.
By this time thee amount of aHUS research findings reported has become quite over whelming but these two sessions show that more patients, other than pure aHUS patients can benefit from complement inhibitions and it it possible to show that complement is being blocked via the HMEC1 assay and also that withdrawal can be uncomplicated too. This test is specific and sensitive enough for the purpose but not yet ready to be done universally.
Prof. Remuzzi got a deserved round of applause from the audience when he appealed to everyone to help get access to be best rare disease treatments by making them more affordable.]
The next talk addressed the issue of transplant supported with a complement inhibitor is more effective if administered prophylactically rather than as a rescue therapy unless accessed quickly. Transplant patient outcomes have been very good for long time in a French study unlike pre-eculizumab availability experience.
A final talk was by an abstract winner whose research showed that in a case study renal function improved in one of her aHUS patients, two years after the patient begun dialysis!
It was left to Prof. Fadi Fakhouri to bring Day 2 to a close by setting out where aHUS has got to in 2022. He said it is no longer a disease of therapeutic issues by one of diagnosis issues and semantics ( needs redefining.) He cited the recent research by aHUS Global Action that has been published. He referred to pure aHUS as a ” Syndrome of Renal TMA” with distinct characteristics.
Given the research reported on at this conference it is evident that much progress has been made.
One more day to go. The patient day.
A reminder that patients can join in on line at this link
ISN provide the following link to the virtual session (via Zoom) of the Patient Day: I.e Day 3 https://us06web.zoom.us/j/87874934774
People who will attend the online session will not need to register.
The session will start at 08.30 a.m. (Italian time) on Saturday 25 June.
{kind=link}