Sometimes it can be confusing being an aHUS patient.
Even to knowing whether you are really an aHUS patient. Even if you have been told by your doctor you have aHUS
You certainly will have had a thrombotic microangiopathy lots of others have had TMAs too and they are not all aHUS patients or are they?.
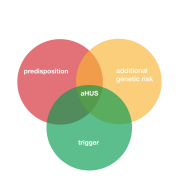
Just look below at some of the images found on the internet to explain what is a confusing situation for patients with aHUS or something else.
If you are an aHUS , or know an aHUS , patient where would you be in any of the following
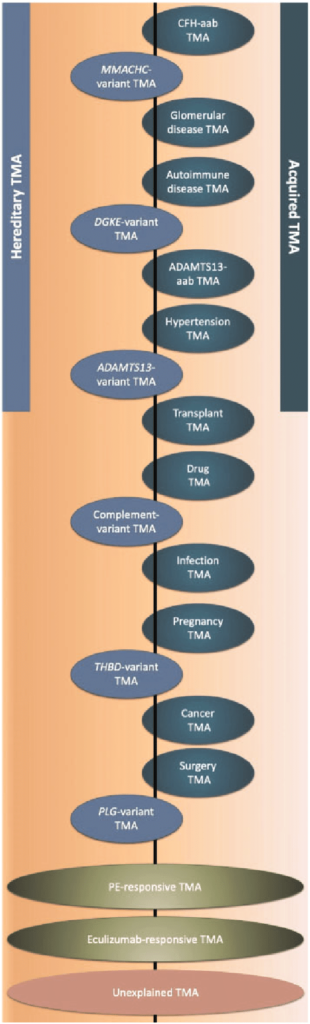
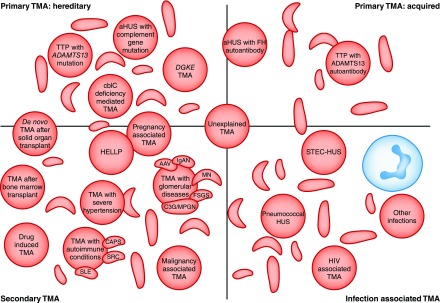
Getting the idea. It is not easy to spot “aHUS” with these illustrations . All show it overlaps or differs from others .
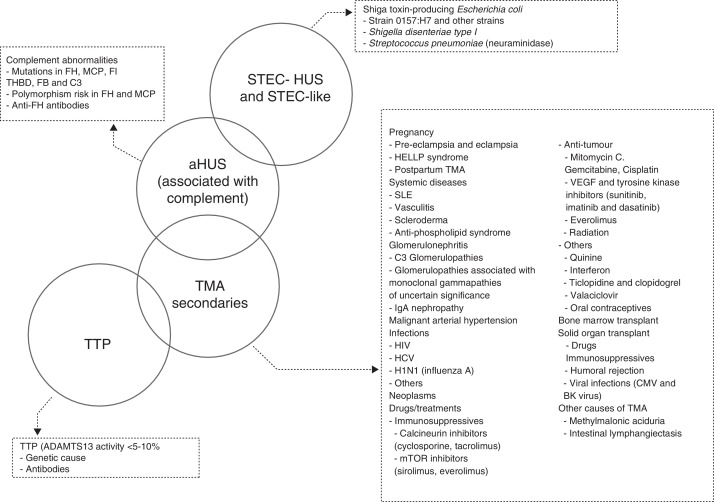
Recently Global Action saw another attempt to illustrate TMAs and where aHUS is within the overall picture . The following illustration from an article abstract by the Aklilu group has TWO primary TMA’s . They are TTP and HUS .
But in this group’s opinion HUS is both STEC-HUS and aHUS . Two HUSs as Conrad Von Gasser claimed!
However STEC HUS can stand on its own, unless the patient has Complement involvement and can be an aHUS patient. Getting a little more complicated.
aHUS can be a primary aHUS which is caused by Complement, or even not due to DGKE , but it can be a whole lot more . See the group’s illustration below.
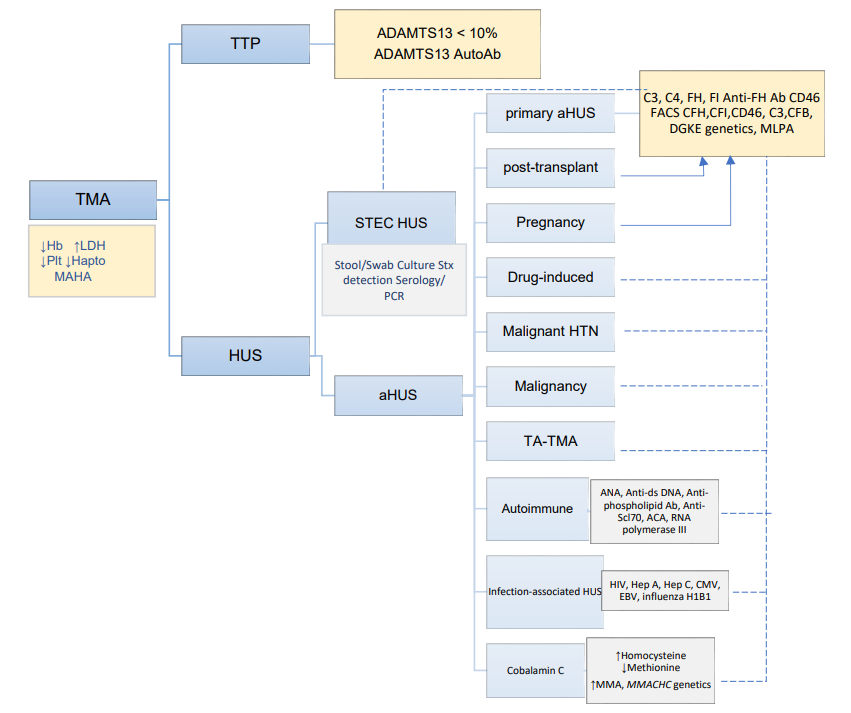
In this chart both post- transplant and pregnancy aHUS patients can have a direct line relationship with Complement and be like a primary aHUS too.
But so can a whole host of other “aHUS” patients with a dotted line link to Complement in some instances and so these can be just like a primary aHUS
So what type of “aHUS” patient seeks out the aHUS alliance Global Action and what type of “aHUS” is advocated for by aHUS alliance Global Action?. Do other non aHUS patient groups advocate for patients when they become primary aHUS patients and need rapid diagnosis and complement inhibitory treatments? Who supports clinical trials for them?
In the Aklilu group article, the patients are cancer patients but, their cancer treatment is leading to a TMA. Could a complement inhibitor tackle that TMA without the drug they need for their cancer being withdrawn?
Cancer patients are advocated for by industrial size and long established patient organisations but would they have interest in a very rare Complement TMA called aHUS. Maybe those patients may be just experiencing an “aHUS like” illness for a short while. And there many more of them than those who have a life with aHUS.
The more patients are reclassified the more complicated this could be become.
aHUS is confusing in so many ways.
Article No. 564
{kind=link}