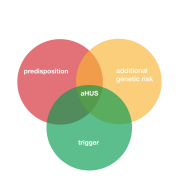
Anyone who can get aHUS can get it any time. That makes sense the disease is just the product of a known or unknown genetic factor and a trigger.
If the year was split into the periods January to April , May to August, and September to December to reflect Winter/spring, Summer and Autumn /Fall around the Winter Summer Solstices then , all things being equal, aHUS onsets should be 33.3% in each of the periods.
It should be as simple as that.
But whenever aHUS alliance Global Action has asked patients what time of the year did they onset with aHUS, other patterns emerge.
Take this one from 2013 based on 38 patient responses on Facebook* to that question, with the year split January to April , May to August , Sepember to December.
The predicted spread would be 33.3% in each period. But these patients reported 18 ( 47% ). 6 ( 16% ) and 14 ( 37% ) respectively.
So , an aHUS onset is much less likely in the summer months than in the rest of year. Making the colder months a time when aHUS is more likely with 84% of cases when 66% of onsets would be expected, if seasonality was not a factor.
The question was asked again in 2022** and out of 62 responses this time the results were for January to April 17 ( 27%), May to August 18 (29%), and September to December 27 (44% ). Different again to the expected spread but the summer months are higher this time and it is Autumn/ Fall to Winter period which has the highest proportion of incidents.
A few years ago similar data was obtained from the aHUS Registry but with a larger sample of aHUS patients. These results for 2012 to 2015 are shown in the table below along with the results outlined above. The statistical significance of the variation from an equal distribution throughout the years has been calculated for each of the survey results. Anything with a value less than .005 would be regarded as significant.
Seasonal Incidence of aHUS and HUX
| Year | Source | Jan to April # | % | May to Aug # | % | Sept to Dec | % | Total | p. value <.005 |
| 2012 | aHUS Registry | 42 | 32 | 41 | 30 | 51 | 38 | 134 | .5067 |
| 2013 | aHUS Registry | 60 | 38 | 52 | 38 | 44 | 29 | 156 | .2917 |
| 2013 | Facebook Group* | 18 | 47 | 6 | 16 | 14 | 37 | 38 | .0523 |
| 2014 | aHUS Registry | 62 | 33 | 54 | 28 | 73 | 39 | 189 | .2355 |
| 2015 | aHUS Registry | 85 | 44 | 55 | 28 | 54 | 28 | 194 | .0082 |
| 2022 | YouTube** | 17 | 27 | 18 | 29 | 27 | 44 | 62 | .2301 |
| Total aHUS | 284 | 37 | 226 | 29 | 263 | 34 | 773 | .0350 | |
| 2018 | Italian tHUS cohort | 12 | 11 | 65 | 62 | 28 | 27 | 105 | .0001 |
Even though there was a Summer dip in onsets not one the surveys showed any significant difference. The closest to being a significant figure is the 2015 aHUS Registry result, ( p= .0082 , p < .005).
So at any time of the year, the chance of having aHUS is pretty much the same.
But what about typical HUS caused by a single trigger E.coli (STEC-HUS) or tHUS
Some results for tHUS are included in the table. The data is for STEC -HUS or tHUS patient onsets over several years reported in a HUS registry in Italy.
These results do reveal a significant difference in onset during the of year.
The Summer period has a very high peak of incidence. ( P= 0001, p< .005.)
It is not for nothing that ecoli is known as the Burger/BBQ disease!
All of this would have little relevance whilst it was believed, quite erroneously, that the incidence of tHUS was ten times the incidence of aHUS.
That would suggest numerically that a tHUS diagnosis would be more likely than aHUS at any time.
But what if the two diseases were much closer in annual incidence?
Would It be unreasonable then to conclude that in the late spring summer and early Autumn period a STEC HUS was the more likely suspect for a TMA?
However in the changeable seasons and colder conditions it would be just as, if not more, likely for a clinician to be suspicious that its aHUS. That could help speed up diagnosis of aHUS patients a bit.
Environmental factors can trigger both HUS and aHUS.
A specific disease is the cause of HUS caused by poor hygiene and undercooked food particulary when the weather is warm.
Many other factors for aHUS, such as winter season diseases might be balanced out by non environmental factors such pregnancy , drugs, transplants to make the chances more evenly spread throughout the year.
If it could help a quicker aHUS diagnosis then this finding may warrant further investigation and wider awareness.
If quality data is available, along with available tHUS data, the aHUS Registry, which has been observing patients for more than 10 years, should now be expected to have a more conclusive opinion on a time of year to have aHUS.
Article No. 589
V
{kind=link}