Nestling in the foothills of the Italian Alps and surrounded by its own parkland, the Villa Camozzi houses the Clinical Research Center for Rare Disease “Aldo e Cele Daccò”. In the early 1990s Professor Giuseppe Remuzzi thought that there was an unmet need for rare disease research and the Centre was the result, thanks to support from the Dacco family who contributed to its renovation. It is a part of the larger Mario Negri Institute, which has a broad disease research portfolio. Professor Remuzzi still leads the Centre and as from July 2018 he has been appointed DIrector of the Mario Negri Institute .

Professor Giuseppe Remuzzi
As the professor was away on business with the Italian Health Ministry, the alliance delegates were welcomed to the Centre in Ranica (Bergamo) at the Villa Camozzi facility by Dr Erica Daina who outlined the development of Centre into the biomedical research unit it has become, and where aHUS research is positioned within its overall activities. The Centre does not treat aHUS patients, but patients are at the heart of what it does. Although not a diagnostic centre, the Centre does perform genetic screening and interprets the results as well as the functional effect of mutations for each patient it screens’
Dr Daina showed the alliance delegates the facilities for patients who may come to the Centre as part of the research work. The day centre ward is run to the same standards as a hospital ward, with eight beds spread over four rooms. It also has very high standard “hotel rooms” for patients to stay when a visit to the Centre needs an overnight stop. Patients and their families are very well looked after.

Dr Raina in one of the patients’ rooms in the Villa.
The Centre also provides a place where individual patients, who call the Centre, can get advice on who they can go to for clinical advice about their rare disease. This is something Prof. Remuzzi believed important for rare diseases patients when the Centre begun and patients felt isolated.
The staff at the Centre come from different medical backgrounds including Nephrology and work in a multi-disciplinary team way. As a research centre its output is publications and presentations at conferences both nationally and internationally (the Magri Negri institute produces an annual report listing its output as a measure of the value it adds).

Agenda for an earlier International Conference about HUS in 2006
The Centre also teaches and runs courses about clinical research , as well as sharing knowledge with a network of hospitals in the Lombardy Region of Italy. Italian health care is regionally based but the Centre has national roles e.g. in the policy of AIFA ( the Italian drug approval body). In 2020 the Centre will be the venue for International Society of Nephrology’s C3G and aHUS Conference for clinicians and patients. (And what a venue!).
Apart from its courses, publications and presentations the Centre adds to its visibility and ability to share knowledge through its website for the Centro di Ricerche Cliniche per le Malattie Rare “Aldo e Cele Daccò” which can be read by clicking here.
The alliance delegates then met with Dr Elena Bresin who talked about the Centre’s. HUS /TTP Registry. Set up in 1996 to understand the characteristics of the aHUS and TTP patients, and then follow them to see the course of the disease and help develop therapeutics. It is the oldest and now perhaps largest of the known aHUS Registries. At June 2018, 1425 patients have been enrolled from 180 participating centres in Italy and in 29 countries internationally, including several countries with an unmet need for aHUS treatment. The Registry is still recruiting and active and is being used to gain greater understanding about patients within the spectrum of aHUS. Dr Bresin went through the recruitment protocol for new registrations. As with all registries the challenge is in the collection of follow up data.

Participating countries in the HUS /TTP Registry
Dr Bresin also showed us some of her,p aHUS research on pregnancy and kidney transplant as well as an international collaboration with Spain, France and UK on the likelihood of renal failure for defects in each Complement component.
Dr Marina Noris ,from the Centre’s Laboratory of Immunology and Genetics of Rare DIseaes gave the alliance delegates a tour of the Laboratory starting with the genetic screening facility. It houses next generation equipment which can look for the known genetic mutations in 55 genes ,and also one that can do it 20,000 genes. Results can be got quickly but the examination and analysis of these can be a challenge and take much longer The Centre also retains a Sanger Sequencing machine to provide quality checks of the other equipment.This illustrates the balance needed between speed and precision of test results.
An example of how the Centre engages with patient organisations was apparent as one of the “robots” used by the Centre for extracting the DNA for testing was funded and provided by the Italian DDD patient organisation. ( But this benefits aHUS patients too.) . Its website contains a database of patient organsations.

The “robot” used in the DNA extraction donated by Progetto DDD Onlus Italy
On the way to meet the Laboratory of Immunology and Genetics of Rare Diseases Team the alliance delegates met with people from the unit that has produced an aHUS mouse model for research as well as someone who, amazingly, has performed kidney transplants on mice for the benefit of kidney transplant research.
In the Laboratory the young, enthusiastic and expert complement investigators gave a briefing of their research including:
CFH and CFHR Hybrid mutation– this is difficult to detect by sequencing, but the laboratory has found a way to detect it using MLPA ( Multiple ligation – dependent probe ) methodology and once revealed they have set about determining whether it has functional significance. It can take months to be precise, but the patient benefits from more personalised care and disease management as a consequence.
Multiple mutations – research here has shown that knowing about all the aHUS predisposing mutations present in an individual patient can enhance understanding of the risk of the disease on-setting; and, for example , in the case of those with MCP plus one or more other mutations would turn a potentially low risk of onset to much more likely following transplant. So, with or without a complement inhibitor such transplant patients would need carefull monitoring.
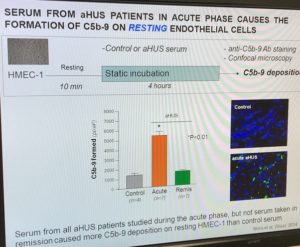
An assay for detecting complement activation– The laboratory has developed a blood test which uses con-focal microscopy to light up aHUS activity on the endothelial cell surface, and which can be done in 6 hours including 2 hours to interpret the result.
Anti-Factor H Autoantibody disease mechanism– AFHA exist in people who may never experience aHUS, so research is being focused on what it is about aHUS patients which makes them more at risk, or what it is about healthy unaffected people that may protect them from aHUS onset.

Elena ( third from left) ,Marina ( first from left) and the team
Although it is now approaching the 30th anniversary of its creation the current centre has modern and up to date facilities in a remarkable setting and is geared up to address questions about aHUS that need still need answering.
The alliance appreciated the time given by all the Centre’s team during the visit and for the Centre’s long history of what it has done, and continue’ s to do, for the global aHUS patient community.
Whistle-Stop Tour of 4 aHUS Centers in the EU: Visits to Three Nations in 6 days (July 2018)
1st Stop: Paris FRANCE
2nd Stop: Newcastle upon Tyne ENGLAND (UK)
3rd Stop: Bergamo ITALY
4th Stop: Milan ITALY

{kind=link}