Some aHUS patients have ended up with end stage kidney failure and need to have a kidney transplant. Such a transplant can trigger another episode of aHUS so complement inhibition is required. Patients ask …
Is there a significant difference in outcome between having a complement inhibitor before or after a kidney transplant?
…so we asked our expert and were told :
“The use of a complement inhibitor, such as eculizumab, can be considered in the management of atypical Hemolytic Uremic Syndrome (aHUS) both before and after a kidney transplant. Pre-transplant use aims to control aHUS activity and minimize the risk of recurrence during the transplant process. Post-transplant, the inhibitor may be continued to prevent aHUS recurrence.
The decision to use complement inhibitors and the timing of administration should be individualized based on the patient’s specific clinical circumstances. It’s crucial to discuss this with the healthcare team managing the aHUS patient, as they can provide personalized recommendations based on the patient’s medical history and current condition.
A healthcare provider may consider giving a complement inhibitor before a kidney transplant in a patient with aHUS based on several clinical circumstances. These may include:
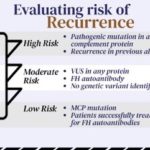
- Active Disease: If the patient has active or recent episodes of aHUS, using a complement inhibitor before transplantation may help control the disease and reduce the risk of recurrence during the transplant process.
- History of Recurrence: If the patient has a history of aHUS recurrence after a previous transplant, preemptive use of a complement inhibitor might be considered to prevent recurrence with the new transplant.
- Severe Manifestations: Patients with severe manifestations of aHUS, such as significant kidney damage or involvement of other organs, may be candidates for complement inhibitors to manage the disease before transplant.
- Genetic Factors: If there is a known genetic mutation associated with aHUS, using a complement inhibitor could be considered, as these cases often have a higher risk of recurrence.
These decisions are made on a” case-by-case basis”, and the healthcare team will carefully assess the individual patient’s medical history, genetic factors, and current clinical status to determine the most appropriate course of action.
Genetic factors associated with a higher risk of aHUS recurrence following a kidney transplant often involve mutations in genes related to the complement system. Mutations in genes such as CFH (complement factor H), CFI (complement factor I), MCP (membrane cofactor protein), CFB (complement factor B), and C3 (complement component 3) are among those associated with a higher risk of aHUS.
Patients with identified pathogenic mutations in these genes may be at an increased risk of aHUS recurrence post-transplant. Genetic testing is typically conducted to identify such mutations in individuals with aHUS, helping healthcare providers assess the risk and make informed decisions regarding the use of complement inhibitors or other preventive measures.
It’s important for individuals with aHUS and their healthcare teams to discuss genetic testing results and tailor the management plan based on the specific genetic factors present.
Identifying low-risk genetic factors for recurrence of aHUS following a kidney transplant can be challenging, as aHUS is often associated with mutations in genes related to the complement system. However, it’s important to note that not all genetic mutations confer the same level of risk for recurrence.
In some cases, secondary aHUS may be triggered by non-genetic factors such as infections or autoimmune conditions. Individuals with aHUS not associated with high-risk genetic mutations might have a lower likelihood of recurrence.
It’s crucial for patients with aHUS and their healthcare teams to conduct thorough genetic testing to identify specific mutations and assess the associated risk. The decision to proceed with a kidney transplant and the use of complement inhibitors will depend on the individual’s genetic profile, overall health, and history of aHUS episodes. This information is best discussed with a knowledgeable healthcare professional familiar with the patient’s case.
Prophylactic (preventive) treatment with complement inhibitors, such as eculizumab, before a kidney transplant in atypical Hemolytic Uremic Syndrome (aHUS) patients aims to minimize the risk of aHUS recurrence during and after the transplant. The decision to use prophylactic treatment is often based on the patient’s clinical history, genetic factors, and other risk considerations.
When aHUS occurs after a kidney transplant, it is considered a medical emergency, and rescue treatment becomes crucial to manage the acute episode and prevent further damage. While rescue treatment can be effective in controlling aHUS, it may not reverse all the damage that has already occurred, potentially leading to ongoing kidney injury.
In summary, prophylactic treatment is designed to prevent aHUS episodes, and receiving rescue treatment after an episode occurs is essential for managing the acute situation. The choice between prophylactic and rescue treatment depends on the individual patient’s risk factors and medical history, and it’s an important decision to be made in consultation with the healthcare team.”
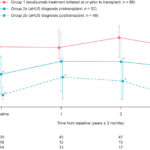
So timing , before or after , can make a difference to health outcomes. Each decision is individualised, but in a way this is similar to the withdrawal of treatment decision involving genetic circumstances , medical history , guide decisions. Except in this case patients are in aHUS remission and are not on treatment but may relapse when a known trigger is introduced.
Those transplant patients given treatment prophylactically might be considered for withdrawal of treatment some time later with no harm done. The patients not treated prophylactically but who are likely to relapse are at risk of harm, which may not be reversed, so they will have to live with less kidney function.
This is an important decision which needs thorough research and input from the patient, each transplant is unique and demands careful thought before going ahead. It is important to have completed all this well before the operation itself particularly for those on a transplant list when the availability of a donor kidney is uncertain. Similarly as for those withdrawing from treatment a care pathway must be put in place for a rapid access to a complement inhibitor if a TMA manifests to eliminate or minimise any harm.
There is also the possibility of patients who had actually had aHUS which destroyed their kidneys but were un or misdiagnosed. The disease may manifest again on transplant. These patients have also to go through the diagnosis process which may delay access to the treatment they now need. Generally these patients have the worst of outcomes, worse than those who are known to have aHUS and rely on rescue therapy; who in turn fare worse than those patients treated prophylactically. Thus answering the agenda question.
Article No. 630
Previous articles on transplants and aHUS
A kidney transplant used to be contraindicated for those predisposed to aHUS. Although it could have been successful for some depending on their genetic susceptibility, most would lose their kidney…
aHUS transplants simplified
Article No. 387 13 October 2020 This website has featured several articles* about the topic of aHUS Transplants and their need for eculizumab support. These articles have provided some of…
CONTINUE READINGaHUS transplants simplified
aHUS Kidney Transplant-More insights
Article No. 378 22 September 2020 aHUS and kidney transplants is an important research topic for aHUS patients with end stage renal failure. aHUS alliance Global Action has featured several…
CONTINUE READINGaHUS Kidney Transplant-More insights

That aHUS transplant question
Article No. 330 8 March 2020 Although it is becoming less of an issue for many these days because the advent of eculizumab/ Ravulizumab saves them from it, but…
CONTINUE READINGThat aHUS transplant question

Transplants, aHUS and eculizumab
The alliance has frequently featured articles about kidney transplants for those with aHUS. It was its top topic identified as a priority for research that matters to aHUS patients ,…
CONTINUE READINGTransplants, aHUS and eculizumab

aHUS Transplants-Abstract Video
The aHUS alliance affiliates put the question: Is there a significant difference in outcome between having a complement inhibitor before or after a kidney transplant? at the top of its…
CONTINUE READINGaHUS Transplants-Abstract Video
Transplant research answers that matter to aHUS patients
These days a kidney transplant may not feature much in the thoughts of new onset aHUS patients, most of them can be saved from a life of chronic end stage…
CONTINUE READINGTransplant research answers that matter to aHUS patients

ERKNET: aHUS and transplants
ERKNET’s website hosts a programme of webinars ( live talks over the internet) about Rare Renal Diseases . The talk today was given by Professor Marius Miglinas , Head of…

Transplant and aHUS Risks
The aHUS Alliance was invited by the aHUS Registry Scientific Board to say what matters most to patients in aHUS research. The alliance’s response to that invitation is well documented…
CONTINUE READINGTransplant and aHUS Risks

Transplantation and aHUS – a top topic
Transplantation of aHUS dialysis patients is a priority and top topic for the aHUS alliance. Transplantation of those with aHUS has been a challenge, not just clinically because of the…
CONTINUE READINGTransplantation and aHUS – a top topic

Before or after , with or without- transplant decisions need data
Anyone, who has been involved in aHUS patient advocacy for some time, will be aware of the special place that those patients, whose aHUS has left them with chronic kidney…

{kind=link}