Very little is heard from ERKNet (European Rare Kidney Disease Network) these days. Global Action used to have articles about its registry.
This EU initiative is more than a registry.
Look at some numbers.
There are according to ERKNet 512 million ( ??) people living in the EU. 30 million of them live with rare diseases and 2 million of those are living with rare kidney diseases.
70,000 of the 2 million are recruited to the ERK Network Registry.
1414 of the 70,000 of the them have TMA kidney diseases. Including some with aHUS/cTMA.
1165 of the1414 are pediatric patients, 249 are adults. As always with registries not all recruits are active in follow up data. So excluding the inactive at 21 May 2026 there are 841 active children and 168 adults.
1009 in total, about 1.4% of all patients in the registry and 0.05% of all with rare kidney disease.
Take it one stage further and they are 0.002% of all who live in the EU.
There are 252 types of kidney disease in total represented in the registry, only the top 25 disease numbers feature in the ERKNet annual report. And aHUS/cTMA numbers are too low to feature separately from all TMA diseases.
Only 8 disease have sub registries dedicated to the disease. One for aHUS/cTMA has not yet even reached the planning stage.
No one knows what the total of TMA patients actually are in the EU but at a prevalence of 5 per million it could be at least 2500 aHUS/cTMA patients. Suggesting that only 1% to 2% of them are registered by ERKNet.
This 1000 TMA cohort get the benefits of:
- Top quality multidisciplinary healthcare
- Diagnosis and treatment guidelines
- Virtual consultancy services
- promoting best knowledge
- new therapies
- supporting research opportunities.
And as everyone with aHUS/cTMA in the EU knows, ERKNet works closely with the patient community. Patients can propose disease research projects. There are no proposals for aHUS/cTMA.
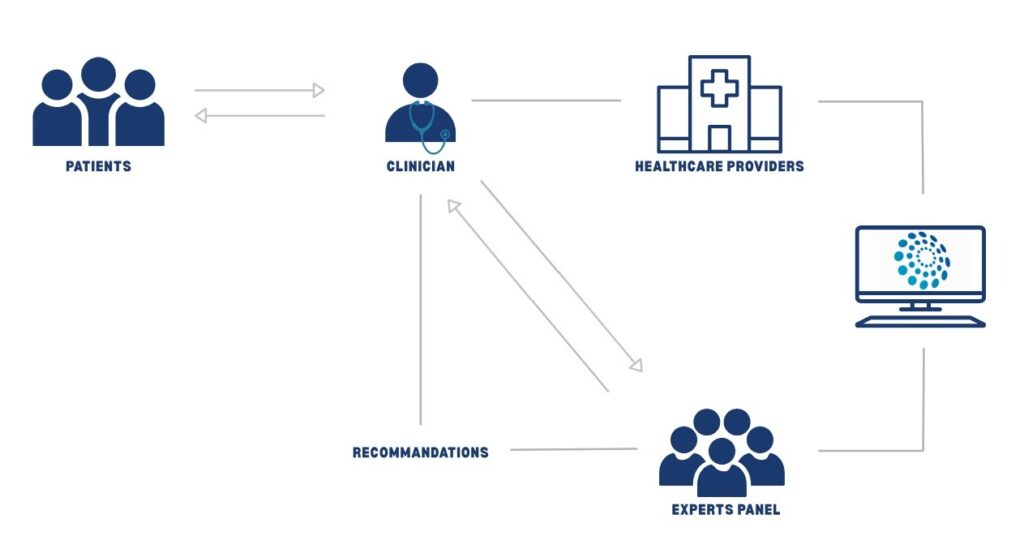
This diagram below illustrates the Clinical Patient Management System set up by the Network. So any patient’s clinician in the EU can call on a wider support system to make the best decisions for the care of their patients.
ERKNet called for research projects from clinicians. No one responded for aHUS/cTMA it would seem.
The Guidelines for aHUS on the website are dated as from 2016 and 2017.
aHUS/CTMA nhas featured as a topic on their webinar education programme on a handful of occasions over the past few years.
There is an article about complement inhibitors use for HUS patients research published in 2025.
The ERKNet HUS cohort used for that was 710 of which 238 had “aHUS” and 472 had “iHUS” (Infectious HUS – the vast majority e.coli related). No transplant patients were included in the study, nor any non complement genetic TMA patients. The article can be read at this LINK .
Most aHUS patients (75%) had received a complement inhibitor, only 18% of Infectious HUS patients were treated with a CI. For a median duration of 16 months and 9 days respectively.
85 of the 238 had a genetic predisposition, 24 had anti-factor H autoantibodies and 105 were idiopathic. 23 were adults, so 90% were children.
Of 182 (178 Ecu, 4 Ravu) who were complement inhibitor (CI) treated 109 discontinued treatment. 19 restarted of whom 8 were re discontinued. A long term treatment withdrawal of just over 92% was achieved. Perhaps success overstated because aHUS transplant patients were excluded from the study and most were children.
After more than seven years only just over half of genetic aHUS patients, 1 in 3 idiopathic aHUS patients and 0% of anti factor H autoantibodies remained on treatment.
Most of the treatment discontinuations were in The Netherlands , France and Ireland. Hardly any in some eastern European countries. Relapses were found to be mild with no permanent damage with early therapy resumption
So this ERKNet study shows the EU:
- has mostly eculizumab use whether due to historic inertia or is done more deliberately.
- has more of a treatment discontinuation strategy than the USA, but that is more likely in western europe than in eastern European countries.
- aHUS patients are a very minor part of the TMA category in the ERKNet Registry
- Research is biased towards the more dominant pediatric cohort in the Registry. Its gender mix does not conform with a female to male mix of 2 to 1 usually found in all age cohort. Before puberty boys are more likely to experience aHUS than girls. More than half of patients in the registry experienced an aHUS/cTMA onset by 5 years of age,
None of this of course is news to the patients in the Registry.
Article No. 803
*TMA includes
- Infectious HUS
- aHUS (including CblC and DGKE)
- TTP
- Lupus TMA
- De novo transplant TMA

{kind=link}